Is
Peyronies Disease Surgery
Necessary to Straighten a Bent Penis?


Peyronies disease surgery will be necessary for some men to straighten their bent penis. For most men, it is not.
Only about 10% of men use surgery to straighten a bent penis. And, most of them could have used non invasive penis traction therapy.
“Penile traction therapy (PTT)
is increasingly being recognized as a viable nonsurgical approach
to
Peyronie’s disease.”
ref: Dr. Shaan A. Setia MD,
penis traction device,
tandfonline.com/doi/abs/10.1080/17434440.2018.1502083?journalCode=ierd20
Quick Links to Common questions and answers:
1. Why avoid surgery?
2. VIDEO: What does a Peyronies disease surgery look like?
3. What are the possible side effects of penis surgery?
4. Do you need Peyronies disease surgery?
5. "Will my cock be 100% straight?"
6. Are there different kinds of Peyronies disease surgery?
7. Are there effective alternatives to surgery?
8. What are the effective non-surgical proven methods of penis straightening?
Why Avoid
Peyronies Disease Surgery?
Peyronies disease surgery is scary for most of us. And, rightly so.
Why?
Because it’s our cock that is being seriously cut up.
Here is a video of a Peyronies disease surgery to straighten a bent penis:
With any penis surgery, sensation will be lost post op simply because so much skin is being cut. That means nerves are being cut.
Why you need to know this:
Nerves carry our physical sensations from our penis to our brain just like electric cords carry electricity to a light bulb. Imagine cutting the cord on an electric lamp. The light goes out until the connection is reformed.
The same is true with nerves in your penis. If you cut a nerve, the electricity (message) does not reach your brain and you can not feel the physical sensation in your penis where the nerve was cut off.
Here’s what makes this so important:
Unfortunately, nerves do not heal quickly, like a cut on your skin, or, a broken bone.
Nerves can take a very long time to heal and reconnect. That could mean 5 - 10 years or more. Unlike a broken bone or a serious cut that can heal in a matter of 6 - 8 weeks, nerves heal slowly. Very slowly.
What Are The Possible Side Effects
of
Peyronies Disease Surgery?
This is a very good question, and, the main reason to avoid Peyronies disease surgery if possible. Almost all of the worst side effects are related to the cut nerves.
There are a number of rather unpleasant possible side effects from a Peyronies surgery that include and are not limited to:
- Impotence
- Lack of sensation
- Inability to orgasm
- Inability to attain or maintain an erection
- Infection
- Future Peyronies bending (about 1/3 of cases)
- Poorer future erections
“....and patients must be warned that long-term worsening of the quality of the erection may occur in up to one-third of cases.”
ref: Asian Journal of Andrology
Long-term results of the surgical treatment of Peyronie's disease with Egydio's technique: a European multicentre study
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3752552/
Do You Need
Peyronies Disease Surgery?
Most men do not.
First of all, Peyronies disease surgery is usually only recommended to men who are in the second phase of Peyronies disease, who have not responded to other therapy, and who’s curvature is so severe that it makes intercourse impossible or terribly painful.

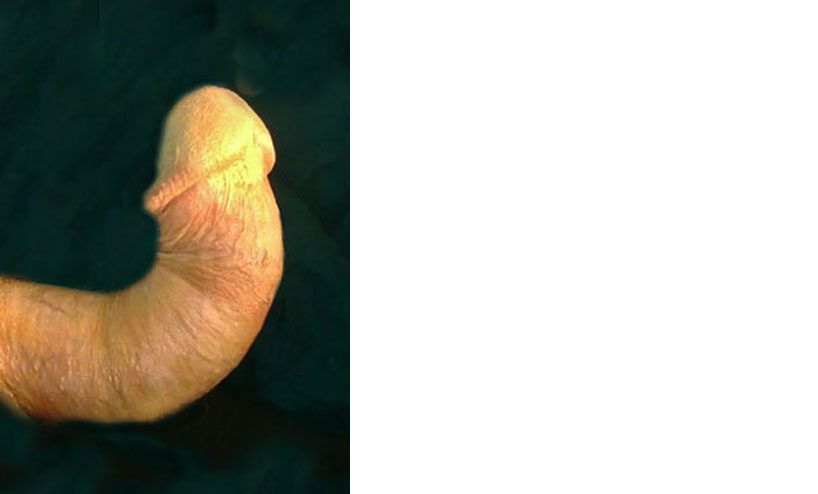
 Severely Bent Penises
Severely Bent PenisesPenis surgery is not something to rush into.
Although most surgeries of this type are successful, they can be a risky business. As you already learned: Only about 10% of Peyronies sufferers will have a surgery.
“About 10% of men have surgery.”
ref: menshealthforum.org
Bent Penis FAQs
https://www.menshealthforum.org.uk/bent-penis-faqs
Here at Bent Penis Org we have come to the conclusion that 99%+ of men can straighten their erection sufficiently for satisfactory intercourse using non-surgical, non-invasive medically recommended methods.
“Will My Cock Be 100% Straight?”
That’s a very good question.
Probably not. Not with Peyronies disease surgery, not with injections, and not with traction.
But, that is of no real significance when you take into account that over half of all men have some degree of penile curvature. Yes, more than half of all men have some bending in their erect shaft.
A small amount of curvature is normal and in no way interferes with intercourse. So, don’t get obsessed with having a perfectly straight erection. Most men don’t.
How Much of a Bend is OK?
As long as you can have sexual intercourse that is comfortable for both you and your partner, any bending or curvature you may have is just meaningless.
You don’t have to be worried about it or concerned with it. Just go enjoy your sex life! Please keep that in mind as you progress with your straightening program.
Now, take a look at this curved erection:
 a small curve usually remains
a small curve usually remainsIf you can achieve anywhere near this kind of straightening, sexual intercourse is never going to be a problem. So, keep that in mind also as you progress with your own straightening program.
Are There Different Kinds
of
Peyronies Disease Surgery?
Yes.
There are four basic ways a penis is straightened with Peyronies disease surgery. The first three involve just surgery. You either shorten the longer side (2 techniques), or, lengthen the shorter side. All erectile function will be left to nature.
The fourth surgical method is placing a prosthetic device inside the penis. You’ll never have a natural erection again. Ever. You’ll use an implanted pump to get an erection. Using a device implant like this has to do with severe erectile dysfunction problems. Although erectile dysfunction often occurs with Peyronies Disease, it is an entirely different topic. We won’t be dealing with it in this article.
Side note: Although erectile dysfunction can come from the changes in the blood vessels when a man has Peyronies disease, it’s also possible to develop a condition called “psychological impotence” when you have PD. This normally resolves itself when the curvature is corrected. So, you must have a very clear discussion with your doctor/surgeon before you consider an implant. Be SURE you need one before you get one.
If you can get erections now, even weak ones, this prosthetic procedure is undoubtedly the wrong choice. Therefore, we will only be discussing the first three methods in this article.
Straightening a Bent Penis
With Surgery
The first method of Peyronies disease surgery used was called the Nesbit procedure. It shortens the erection.
 Nesbit Procedure
Nesbit Procedure
The Nesbit Procedure shortens the longer side of the bend so that the penis will come out straight again during erection.
This
will make the new erection anywhere between 1/4 inch and a whopping 2
inches shorter during erection. Yes, 2 inches shorter. It all depends
upon how severe the curve is and how long the penis was to start with.
One half inch shorter is average.
The second, and newer, similar method is called 16 Dot Plication (folding).
 16 Dot Plication
16 Dot Plication
16 Dot Plication uses sutures (stitches) to fold together some of the internal tissue, instead of cutting out the plaque and resewing the tissue, to straighten the shaft.
It looks kind of like lacing up a boot, although it is not quite the same.
16 Dot Plication is quite effective. The internal stitching does leave small bumps in the shaft because the stitches are not absorbed, but they do not seem to interfere with patient satisfaction. It is less invasive than the Nesbit procedure and poses less post operative complications.
However, his method of penis straightening seems better suited to men with congenital curvature (from birth) rather than Peyronies disease. For men with PD the Nesbit procedure may be preferable due to the fact that the sutures (stitches) all by themselves may not be strong enough to prevent future recurrence of the bend.
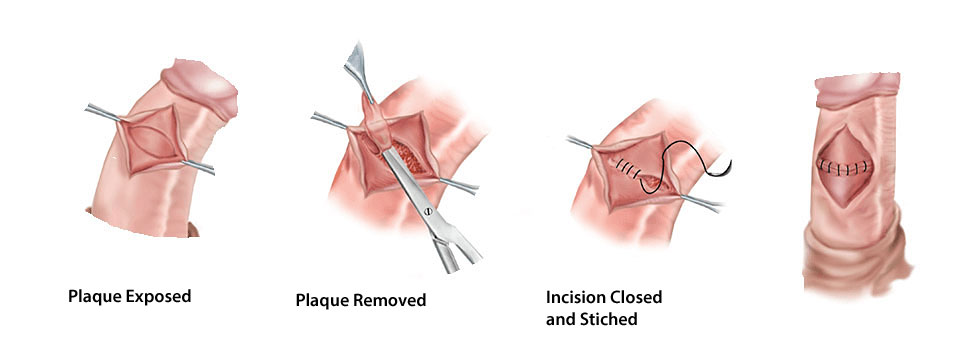
The third method used is called Plaque Incision and Grafting.
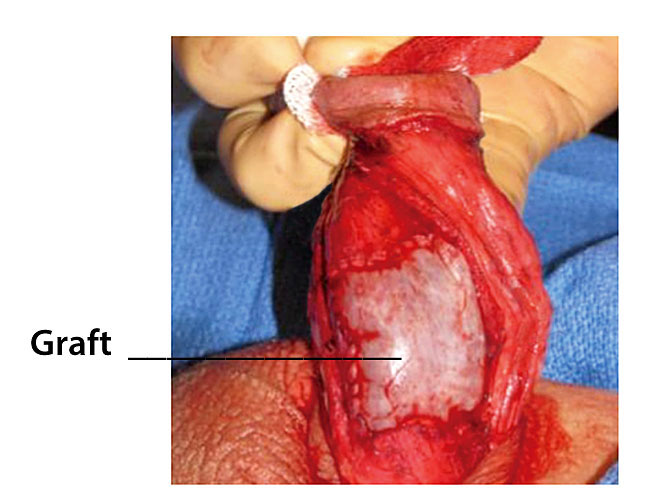 Plaque Incision and Grafting
Plaque Incision and Grafting
Plaque Incision and Grafting is much more popular because it does not shorten the erection. Rather, the shorter side is cut and a graft is placed there to make the shortened side longer. This enables a man to retain all of his former erectile length.
The grafting material used is tissue from another part of the body, from a donor (human or animal), or, most commonly, a synthetic material (made from human or animal sources). These synthetic tissue grafts act as supportive structures for the body to grow new, healthy tissue on while the grafts are slowly absorbed by the body.
Unfortunately, this procedure comes with the risk of worsening already existing erectile dysfunction.
"There is a risk, however, that this technique could make ED (erectile dysfunction) worse if it already exists."
ref: Urology Care Foundation
How is Peyronie’s Disease Treated?
https://www.urologyhealth.org/urologic-conditions/peyronies-disease/treatment
Alternatives
to
Peyronies Disease Surgery
Now, there are a number of alternative medical treatments to Peyronies disease surgery that have been tried and some are still being employed.
Penis Traction Therapy (PTT)
- We have found the research showing this to be the #1 Safest and Most Effective treatment 99% of the time
Oral Drugs
- Oral vitamin E
- Potassium amino-benzoate ("Potaba")
- Tamoxifen
- Colchicine
- Carnitine
Penile Injections
- Collagenase injections (Xiaflex)
- Verapamil injections
- Interferon injections
Other Methods
- Ultrasound
- Radiation
- Shock-waves
- Heat
- Verapamil on the skin
“Treating the penis with ultrasound, radiation, shock-waves, heat, and
verapamil on the skin are also being studied. These, for the most part,
are not proven and are not recommended by experts in the field.”
ref: Urology Care Foundation
How is Peyronie’s Disease Treated?
https://www.urologyhealth.org/urologic-conditions/peyronies-disease/treatment
The ONLY TWO alternative methods to Peyronies disease surgery that have proven to give acceptable reliable results are penis traction therapy, and Xiaflex injections. Penis traction therapy has proven to be the safest and most effective.
Let’s Take a Detailed Look
at
The Proven Non-Surgical Methods
Outside of Peyronies disease surgery, you now know there are only two medically recommended treatments to straighten a bent penis that have proven to be predictably successful enough for a man to return to normal sexual intercourse.
These are Xiaflex injections and Penis Traction Therapy (PTT).
Let’s take a look at both of these methods:
Xiaflex Injections
Almost all men would prefer to avoid a Peyronies disease surgery. Xiaflex is the patented trade name for the drug: collagenase clostridium histolyticum. It is the only FDA approved injection for Peyronies Disease treatment.

It is sometimes called “The Rich Man’s Cure” because the price for a full set of injections and the doctor’s fees runs about $30,000. Yes, that is thirty thousand dollars.
Although Xiaflex is far less invasive than a penis surgery, Xiaflex does come with some serious possible side effects of it’s own including:
“Penile fracture (corporal rupture) or other serious injury to the penis.
After treatment with XIAFLEX®, blood vessels in your penis may also break, causing blood to collect under the skin (hematoma). This could require a procedure to drain the blood from under the skin
Symptoms of corporal rupture or other serious injury to your penis may include:
- a popping sound or sensation in an erect penis
- sudden loss of the ability to maintain an erection
- pain in your penis
- purple bruising and swelling of your penis
- difficulty urinating or blood in the urine”
ref: Xiaflex.com
For the full list of possible side effects, please go to the Xiaflex.com website.
Penis Traction Therapy (PTT)

The first and most significant benefit of penis traction therapy over Peyronies disease surgery, or the injections, is: PTT comes with NONE of the possible surgical or Xiaflex injections side effects. None.
- PTT is safe when used properly
- PTT is medically endorsed and doctor recommended in 29 countries worldwide
The one drawback to penis traction therapy is the time it takes. Usually 6+ months. The penis traction device must usually be worn 6 days a week for 4 - 6 hours each day.
Fortunately the device is easy to use. It can be worn under your normal clothing while you go about your normal daily activities. (Unless of course you are a professional athlete or have some other such highly physical profession. Then you’d need to use it later in the day.)
If you need a week off from it here and there, no problem. Just remember to start using it again regularly.
Consistent use is the key with penis traction therapy.
Is Peyronies Disease Surgery
The Best Choice?
 hourglass penis
hourglass penisIn most cases surgery is not the recommended choice to fix a bent penis caused by Peyronies disease or any other cause.
Yes, penis surgery is necessary in some cases. And, it is the only option for an hourglass penis.
But, Peyronies disease surgery is usually only recommended for a bent penis when other less or non invasive methods have failed.
“Surgery...for Peyronies disease.... is usually only recommended in severe cases for patients who fail to respond to non-surgical therapy and have curvature for longer than 12 months.”
ref: University of California San Francisco,
Surgical Treatment for Peyronie's Disease
https://www.ucsfhealth.org/education/surgical_treatment_for_peyronies_disease
The Safest and Most Effective medically recommended method of penis straightening has proven to be simple Penis Traction Therapy (PTT). PTT can effectively straighten a bent penis 99% of the time.
Be Well.....
~ William
References
Aaronson DS, Shindel AW. U.S. national statistics on penile fracture. J Sex Med. 2010;7(9):3226. doi: 10.1111/j.1743-6109.2010.01879
Austoni E, Colombo F, Mantovani F, Patelli E, Fenice O. Radical surgery and conservation of erection in Peyronie's disease. Arch Ital Urol Androl. 1995;67(5):359–364. (Ita)
Brake M, Keller H, Lamade F, Groh R, Horsch R. Operative Korrektur der Penisdeviation. Surgical correction of penile deviation. Nesbit vs. Schroeder-Essed method]. Urologe A. 1999;38(3):264–269. doi: 10.1007/s001200050279
Chitale S, Morsey M, Swift L, Sethia K. Limited shock wave therapy vs sham treatment in men with Peyronie's disease: results of a prospective randomized controlled double-blind trial. BJU Int. 2010;106(9):1352–1356. doi: 10.1111/j.1464-410X.2010.09331
B.L. Dalkin, M.F. CarterVenogenic impotence following dermal graft repair for Peyronie’s disease. J Urol, 146 (1991), pp. 849-851
P.H. Egydio, A.M. Lucon, S. ArapA single relaxing incision to correct different types of penile curvature: surgical technique based on geometrical principles. wiley.com/doi/full/10.1111/j.1464-410X.2004.05220
Essed E, Schroeder FH. New surgical treatment for Peyronie disease. Urology. 1985;25(6):582–587. doi: 10.1016/0090-4295(85)90285-7
Gelbard MK, Dorey F, James K. The natural history of Peyronie's disease J Urol. 1990;144(6):1376–1379
Gholami SS, Lue TF. Correction of penile curvature using the 16-dot plication technique: a review of 132 patients. J Urol. 2002;167(5):2066–2069. doi: 10.1016 S0022-5347(05)65085-9
Gur S, Limin M, Hellstrom WJ. Current status and new developments in Peyronie’s disease: medical, minimally invasive and surgical treatment options. Expert Opin Pharmacother 2011;12:931-44
K. Hatzimouratidis, I. Eardley, F. Giuliano, D. Hatzichristou, I. Moncada, A. Salonia, et al.EAU guidelines on penile curvature
Eur Urol, 62 (2012), pp. 543-552
Hauck EW, Mueller UO, Bschleipfer T, Schmelz HU, Diemer T, Weidner W. Extracorporeal shock wave therapy for Peyronie's disease: exploratory meta-analysis of clinical trials. J Urol. 2004;171(2 part 1):740–745. doi: 10.1097/01.ju.0000108060.30363.8d
G.L. Hsu, C.H. Hsieh, H.S. Wen, P.Y. Ling, S.Y. Chen, H.M. Huang, et al.Formulas for determining the dimensions of venous graft required for penile curvature correction
Int J Androl, 29 (2006), pp. 515-520
Imbeault A, Bernard G, Ouellet G, Bouhout S, Carrier S, Bolduc S. Surgical Option for the Correction of Peyronie's Disease: An Autologous Tissue-Engineered Endothelialized Graft. J Sex Med. 2011;8(11):3227–3235. doi: 10.1111/j.1743-6109.2011.02374
Kadioglu A, Akman T, Sanli O, et al. Surgical treatment of Peyronie's disease: a critical analysis. Eur Urol 2006;50:235-48
Kadioglu A, Sanli O, Akman T, Ersay A, Guven S, Mammadov F. Graft materials in Peyronie's disease surgery: a comprehensive review. J Sex Med. 2007;4(3):581–595. doi: 10.1111/j.1743-6109.2007.00461
Kelami A. Congenital penile deviation and straightening of the penis using the Nesbit-Kelami technique. Urol Int. 1985;40(5):267–268. doi: 10.1159/000281096
Kovac JR, Brock GB. Surgical outcomes and patient satisfaction after dermal, pericardial, and small intestinal submucosal grafting for Peyronie's disease. J Sex Med. 2007;4(5):1500–1508. doi: 10.1111/j.1743-6109.2007.00453
L.A. Levine, A.L. Burnett. Standard operating procedures for Peyronie’s disease
J Sex Med, 10 (2013), pp. 230-244
Levine LA, Greenfield JM, Estrada CR. Erectile dysfunction following surgical correction of Peyronie’s disease and a pilot study of the use of sildenafil citrate rehabilitation for postoperative erectile dysfunction. J Sex Med 2005;2:241-7
L.A. Levine. The clinical and psychosocial impact of Peyronie’s disease Am J Manag Care, 19 (Suppl. 4) (2013), pp. 55-61
Martinez D, Ercole CE, Hakky TS, et al. Peyronie’s Disease: Still a Surgical Disease. Adv Urol 2012;2012:206284
Ralph D, Gonzalez-Cadavid N, Mirone V, Perovic S, Sohn M, Usta M, Levine L. The management of Peyronie's disease: evidence-based 2010 guidelines. J Sex Med. 2010;7(7):2359–2374. doi: 10.1111/j.1743-6109.2010.01850
Ralph DJ, al-Akraa M, Pryor JP. The Nesbit operation for Peyronie's disease: 16-year experience. J Urol. 1995;154(4):1362–1363. doi: 10.1016/S0022-5347(01)66862-9
S. Sansalone, G. Garaffa, R. Djinovic, S. Pecoraro, M. Silvani, G. Barbagli, et al. Long-term results of the surgical treatment of Peyronie’s disease with Egydio’s technique: a European multicentre study
Asian J Androl, 13 (2011), pp. 842-845
Sassine AM, Wespes E, Schulman CC. Modified corporoplasty for penile curvature: 10 years' experience. Urology. 1994;44(3):419–421. doi: 10.1016/S0090-4295(94)80106-1
Savoca G, Trombetta C, Ciampalini S, et al. Long-term results with Nesbit’s procedure as treatment of Peyronie’s disease. Int J Impot Res 2000;12:289-93
Schwarzer U, Sommer F, Klotz T, Braun M, Reifenrath B, Engelmann U. The prevalence of Peyronie's disease: results of a large survey. BJU Int. 2001;88(7):727–730. doi: 10.1046/j.1464-4096.2001.02436
Syed AH, Abbasi Z, Hargreave TB. Nesbit procedure for disabling Peyronie’s curvature: a median follow-up of 84 months. Urology 2003;61:999-1003
C. Van Dr Horst, F.J. Martinez Portillo, C. Seif, P. Alken and K.P. Junemman. Treatment of penile curvature with Essed-Schröder. Treatment of penile curvature with Essed-Schröder
tunical plication: aspects of quality of life from the
patients’ perspective.Departments of Urology, University Hospital Schleswig-Holstein/Kiel and Mannheim, Germany, wiley.com/doi/pdf/10.1111/j.1464-410X.2004.04566
Yachia D. Incisional Corporoplasty for the Correction of Peyronie's Disease Caused Penile Curvature. In: Levine LA, editor. Peyronie's Disease: A guide to clinical management. Totowa, New Jersey: Humana Press; 2007. pp. 161–174
Yachia D. Modified corporoplasty for the treatment of penile curvature. J Urol. 1990;143(1):80–82
Zargooshi J. Sexual function and tunica albuginea wound healing following penile fracture: An 18-year follow-up study of 352 patients from Kermanshah, Iran. J Sex Med. 2009;6(4):1141–1150. doi: 10.1111/j.1743-6109.2008.01117
Recent Articles
-
The Bent Penis Disease - 2025
 A bent penis disease does not exist. Yes, we have all heard of Peyronies disease. But, that is actually not a "disease"
A bent penis disease does not exist. Yes, we have all heard of Peyronies disease. But, that is actually not a "disease" -
The Bent Penis Cure
 Is there a bent penis cure? Yes. In fact there are a few. However, some come with serious possible side effects.
Is there a bent penis cure? Yes. In fact there are a few. However, some come with serious possible side effects. -
The 6 Bent Penis Causes
 There are 6 bent penis causes: Genetic, Peyronies Disease, FracturedPenis, Stretching, Autoimmune Disease, Circumcision
There are 6 bent penis causes: Genetic, Peyronies Disease, FracturedPenis, Stretching, Autoimmune Disease, Circumcision -
What is a Banana Penis?
 A banana penis is a simple curved penis. It’s not a slight bend. It’s not a severe bend like Peyronies disease. But, it
A banana penis is a simple curved penis. It’s not a slight bend. It’s not a severe bend like Peyronies disease. But, it -
How to Fix a Bent Penis Naturally, Without Surgery
 To fix a bent penis caused by Peyronies disease or, a congenital curvature (one you are born with), traction is the #1
To fix a bent penis caused by Peyronies disease or, a congenital curvature (one you are born with), traction is the #1 -
Straighten a Curved Penis Naturally, Without Surgery
 Is it a curved penis or is it Peyronies Disease? Either way, you can straighten and fix it without surgery 99% of the
Is it a curved penis or is it Peyronies Disease? Either way, you can straighten and fix it without surgery 99% of the -
Why Are Some Penises Bent?
 Why are some penises bent? There are generally 4 reasons: Peyronies Disease, genetics, autoimmune disorder, disease and
Why are some penises bent? There are generally 4 reasons: Peyronies Disease, genetics, autoimmune disorder, disease and -
Penis Stretching to Straighten a Bent Penis
 Penis stretching is actually the safest and most effective method to straighten a bent penis if it is done correctly.
Penis stretching is actually the safest and most effective method to straighten a bent penis if it is done correctly. -
How to Fix a Curved Penis - the 3 Most Effective Methods
 Learn how to fix a curved penis with the 3 best medically endorsed methods. Surgery may not be necessary.
Learn how to fix a curved penis with the 3 best medically endorsed methods. Surgery may not be necessary. -
Penis Traction Therapy Medical Doctor Recommendations
 Penis traction therapy to straighten a bent penis caused by Peyronies disease is becoming the first line treatment.
Penis traction therapy to straighten a bent penis caused by Peyronies disease is becoming the first line treatment. -
Straighten A Bent Penis Naturally
 Even a severely bent penis can be straightened naturally, without surgery 99.99% of the time. Medically Approved
Even a severely bent penis can be straightened naturally, without surgery 99.99% of the time. Medically Approved -
Which Penis Traction Devices Are Best? Review
 Penis traction reviews. The best devices are: 1) Made with medical grade materials. 2) Class 1 medical devices. 3)
Penis traction reviews. The best devices are: 1) Made with medical grade materials. 2) Class 1 medical devices. 3) -
Penis Traction and Peyronies Disease
 Penis traction works. 99% of the time. No Surgery Necessary. OK? A bent penis surgery is usually not needed
Penis traction works. 99% of the time. No Surgery Necessary. OK? A bent penis surgery is usually not needed -
Signs of Erectile Dysfunction
 What are the signs of erectile dysfunction? You already know. Right? But, is it erectile dysfunction, or, normal aging?
What are the signs of erectile dysfunction? You already know. Right? But, is it erectile dysfunction, or, normal aging?
New! Comments
The Bent Penis Org authors and I would love to hear what you have to say about the pages you have read here. Your thoughts are important to us. If you can, please leave us a comment in the box below. Thanks! ~ William